Duration of fasting
More doesn't mean better

Fasting has been growing increasingly more popular in recent years, and there are so many new regimens that their abundance can disorient a beginner. What’s the best way to choose a regimen for yourself?
First of all, we need to decide what we want to achieve. If your goal is to prevent diseases and tonify the body, good results will be delivered by intermittent fasting using the 5:2 water fasting, 6:1 dry fasting (I. Khoroshilov), or one-meal-a-day (OMAD) regimens. They allow the digestive tract to rest periodically and help keep weight under control. A one-time three-day water fast increases the tone and ability of a healthy person to endure physical activity (T. Kustarev 1999). These short intermittent abstinence regimens are safe, have simple universal protocols, and do not require specific entry and exit rules.
But if we want to use fasting as therapy to help cope with chronic disease, a long-term fast is optimal. It requires a more serious approach and adherence to a number of rules, and the time of abstinence from food is of critical importance. Sometimes, during fasting, patients follow the principle of “the longer the better,” thereby subjecting their bodies to unnecessary endurance tests. A healthy person is likely to endure complete water fasting for 30-40 days without undesirable consequences, but should one undertake it and what benefits will it produce? Let’s dwell on this in more detail, but first, let’s make an important note.
Important: For safety reasons, long-term therapeutic fasting should not be undertaken independently. Even the doctors who most ardently support this method do not recommend its application without a specialist’s supervision. However, there is no consensus on the time limit for fasting at home. Russian practitioners have two contradicting opinions. Prominent scientist and nutritionist Igor Khoroshilov (widely known for being the first to substantiate the use of dry fasting in clinical practice in 1994), recommends medical supervision for water fasts that last over 3 days. Igor Khoroshilov considers 1 day (36 hours) to be the optimal period for home dry fasting, but notes that it should not exceed 3 days. A different opinion on this matter is expressed by Dr. Sergei Filonov in his book 20 Questions and Answers about Dry Fasting, which we recently published in English. If there are no concomitant pathologies, then dry fasting at home can last for up to 5 days, he claims. In our opinion, this disparity in recommendations is due to these doctors’ different approaches to the level of acceptable risk.
Medical supervision during prolonged fasting is required for at least two reasons. The first reason is that the treatment process (both during dry and water fasting) often goes through a stage of exacerbation of chronic diseases, for example, a renal colic. If such an exacerbation occurs, the doctor must adequately assess the severity of the situation and decide whether to continue or interrupt the course of treatment. The second reason is the need to correctly determine the time to break the fast, which is individual for each patient. Medical experience, which will be discussed below, shows that an increased therapeutic effect does not always correlate with an increase in the duration of fasting. Sometimes it is advisable to limit yourself to relatively short periods.
Since the 1960s, after the successful results obtained by Yuri Nikolaev in working with neuropsychiatric patients, the therapeutic fasting method began to be widely introduced into clinical practice in the USSR. This method was used by doctors of various specialties:
psychiatrists, pulmonologists, gastroenterologists, cardiologists, dermatologists, hematologists.
The results they obtained confirmed a pattern first discovered by Franz Xaver Mayr in the early 20 th century: the patient goes through 3 stages during fasting, and the therapeutic effect depends on which one of them was achieved by the time that the fast has been broken. The stage the patient had reached is crucial in the decision to break fasting, rather than how many days the patient has spent without food.
Yuri Nikolaev provided a detailed description of clinical signs during fasting (1973). On this basis, doctors determine what stage the patient has reached and when treatment should be completed. However, a prepared person can do it on their own. To obtain a therapeutic effect, in Yu. Nikolaev’s experience, it is highly desirable to wait until the last, third stage is completed.
A continued fast loses its therapeutic value, and even poses a threat to life, since the body begins to consume vital tissues and organs. What are the stages of fasting, and how are they manifested?
Yuri Nikolaev describes the stages that a fasting person goes through (1969):
Stage 1 (food arousal). During this stage, which usually lasts 2–4 days, the patients are irritated by any food signals: its sight and smell, speaking of food, the sound of tableware, etc. Food signals cause salivation, stomach rumbling, an empty sensation in the stomach. In some patients, general disinhibition and an increase in tendon reflexes are observed. Quality of sleep worsens, irritability increases, and the patient is in a generally bad mood. Body weight drops rapidly (weight loss is up to 1 kg/day). Thirst is usually insignificant. Patients drink very little (300–500 gr.). Despite this, the urine output increases. Excretion of feces after an enema is quite prolific. The feces contain remnants of previously eaten food and have a normal color and odor. Blood pressure remains unchanged in most patients. The pulse quickens somewhat (by 5-10 beats per minute) and becomes unstable, breathing also quickens.
Stage 2 (increasing acidosis). On days 3-5 of abstinence from food, the hunger sensation usually decreases, and sometimes completely disappears. The smell and sight of food ceases to attract patients, while thirst usually intensifies at this time. There is an increasing general psychomotor retardation in most patients. At times, especially in the morning, some of the patients complain of headache, dizziness, nausea, feeling of weakness. However, these phenomena are largely reduced or disappear completely after a walk, warm-up outside, alkaline mineral water intake.
During a physical examination, patients present with increasing amounts white or gray tongue plaque, dryness of the tongue and lips, mucus on the teeth, an acetone smell from the mouth, skin dryness and pallor. The abdomen becomes retracted, intestinal loops are easily palpated. Patients note a decrease or disappearance of the empty stomach feeling and stomach rumbling. The pulse slows down, and blood pressure decreases slowly and gradually. Breathing becomes deeper and more rare. Vesicular respiration increases in the lungs. The pupils are slightly constricted. In some patients, there is a slight exacerbation of symptoms of concomitant chronic somatic diseases that are in a latent state. For example, soreness in the gallbladder region and slight jaundice in patients with cholecystitis; painful joints in patients with rheumatism, an increased sputum production in patients with bronchitis.
The daily body weight loss quickly decreases to about 300-500 g. The amount of feces excreted after an enema also declines, it looks like dark lumps the size of a hazelnut, and is almost odorless. It consists of food remnants, bile pigments, mucus, bacteria and flakes of the intestinal mucosa. The specific gravity of urine increases further (up to 1025–1030 g). Mucus and a large amount of salts appears in it, and the number of leukocytes increases.
There are no specific changes in the full blood count. Blood biochemistry tests demonstrate an increase in urine acetone, a decrease in blood sugar (from 105–95 to 80–65 mg%), a drop in reserve alkalinity (from 49–62 to 28–45 vol%), an increase in ammonia nitrogen in urine (from 0,6-0.9 to 1.0-1.5 mg%) accompanied by a decrease in the amount of total nitrogen in urine.
All the above phenomena that characterize the second stage in different patients increase with different intensity up to day 7-10 of fasting, after which the patients’ condition changes very quickly, even dramatically, and the third stage begins.
Stage 3 (adaptation). Sometimes within a span of one day or even several hours, often at night, a dramatic change occurs in the patient’s condition. It is the so-called acidotic crisis.
There is a significant improvement in overall well-being. The feeling of physical weakness decreases or completely disappears, the patient is invigorated and their mood improves, various unpleasant sensations in the body cease, and the previously exacerbated manifestations of concomitant somatic diseases disappear.
In some patients, this improvement proceeds in a wave-like manner, and the moments of improvement are short at first, and become increasingly longer with time. Starting at this point, the tongue begins to clear of plaque (first the tip and edges, then the middle). Complexion improves, a pallor disappears, sometimes a blush appears. At the same time, the odor from the mouth and from the skin disappears, and sweating decreases.
Diuresis increases slightly, and the specific gravity of urine decreases again, the amount of salts, mucus and leukocytes declines. The subcutaneous fat layer is sharply reduced, and there is a significant overall weight loss. The stomach is retracted. Palpation is usually painless, the liver and spleen are not palpable, and intestinal peristalsis is not observed.
A significant increase in spontaneous gastric secretion is noted.
The heart sounds in most patients become more sonorous, the pulse is rare.
Most patients have present with mild sinus bradycardia on the electrocardiogram. Daily weight loss becomes minimal, and is equal to 100-200 g per day.
In some patients, the blood count shows an insignificant decrease in the number of leukocytes (by 500-600, compared with the initial level).
Biochemical tests show an increase in blood sugar up to 90-100 mg%, an increase in reserve alkalinity of up to 40-50 vol.%, a decrease or complete disappearance of acetone and an increased amount of ammonia in the urine, a decrease in urine titration acidity.
The electroencephalogram shows low electrical activity in all leads, a very weak reaction to external stimuli, the curve pattern is monotonous.
The patients’ mental state usually shows a significant improvement, their mood is better, anxiety disappears, they grow interested in their surroundings, and are included in the life of the ward.
In many patients with a hypochondriacal syndrome, who experienced a decrease in cenesthopathy during the second stage, present with their complete cessation in the third stage and a disappearance of a fixation on these sensations.
Patients with hallucinatory paranoid syndrome become more relaxed and accessible, their delusions and hallucinations gradually vanish, as if fading into the background, lose their relevance and significance for patients.
In some cases, they disappear completely, although a critical attitude towards them in patients is infrequent.
Lethargy and apathy decrease in patients with a simple form of schizophrenia, they become more mobile, alert and proactive, they become involved in work processes, begin to come in contact with others, take an interest in the life of their loved ones, and discover correct social attitudes.
In patients with a catatonic form, tension and negativism decrease. They begin to get out of bed, go for walks, show less resistance to therapeutic procedures (enemas, baths, massage, etc.), and sometimes actively participate in them. Their gaze becomes meaningful.
Some patients, who were previously in a state of catatonic stupor and mutism, begin to answer questions and get out of bed independently.
The duration of this stage is subject to the greatest individual variation. It depends on the general state of the patient’s reactivity, nutritional status, the condition of the cardiovascular system, mental state, etc. This stage ends dramatically, with the appearance of a strong appetite, which in most cases occurs on the day 20-30 of abstinence from food. The tongue is completely cleared of plaque; it becomes red and moist.
By this time, the patients’ sleep deteriorates again, many patients dream of tasty food, they wake up on a pillow that’s wet with saliva in the morning. Slight irritability sets in again, the feeling of weakness intensifies. At the same time, patients very often experience a slight increase in heart rate and blood pressure, both maximum and minimum (by 10-15 mm Hg). The amount of blood sugar decreases from 72-80 to 68-71 mg per 100 ml. At this point, restorative nutrition should begin.
Clinical signs of the completion of fasting are as follows: an appetite appears, complexion clears up, the tongue is cleansed from plague, bad breath disappears and a minimal amount of feces come out after an enema.
*****
The acidotic crisis described above reflects the adaptation of the body to internal (endogenous) nutrition. According to Yu. Nikolaev, this launched the synthesis of glycogen from fat, which is not typical for a person on a regular diet, since sufficient quantities of carbohydrates are usually supplied with food. Fat oxidation is more complete in the presence of the produced glycogen, leading to a decrease in acidosis and, as a result, to an improvement in well-being.
Russian doctors who adhere to Yu. Nikolaev’s guidelines attach great importance to the acidotic crisis, considering it a required condition for obtaining a therapeutic effect. Yuri Nikolaev himself recommended not only going through the acidotic crisis, but also completing the third stage of fasting. Nevertheless, he states that sometimes, due to a number of circumstances, it is necessary to interrupt fasting and start feeding patients prior to the end of the third stage. This does not exclude the possibility of a positive treatment result, provided that the acidotic crisis is passed.
The processes that go on in the body during fasting are far from being fully understood.
This is probably why we were unable to find clearly reasoned explanations in literature of the reasons for the association of the therapeutic effect with the onset of an acidotic crisis. Today we have to be content with the fact that the existence of this connection is confirmed by the experience of doctors of various specialties who have used fasting as a method of treatment.
Doctors often seek to reduce the duration of fasting, while maintaining its therapeutic effect. For example, it was noted in the treatment of asthma (I. Belyaeva, 1992) that as the period of abstinence from food increased in asthma patients, side effects (weakness, palpitations, dizziness) and the risk of developing an acute viral infection also increased. Thus, the fasting course for this group of patients was limited to 14 days.
In the treatment of alimentary constitutional obesity (G. Dorokhov, 1996), long fasts were found to impair immunological parameters: they decrease the number of T-lymphocytes, the concentration of the C3 complement component in the blood serum, etc. Therefore, in this case, the fasting course was limited to 14 days, and in the presence of concomitant internal organ diseases – to 8-9 days.
However, even when trying to shorten the fast as much as possible, the researchers considered the acidotic crisis a necessary condition for achieving a therapeutic effect. One of the ways to shorten the duration of treatment is dry fasting. This type of fasting accelerates the onset of an acidotic crisis, which occurs after 2-4 days, rather than 6-9 days, as during water fasting. The combined fasting method, which consists of a 3-day dry fast and a subsequent 10 to 14-day water fast, became popular among Russian doctors (I. Khoroshilov 1994, S. Osinin, 1993, S. Filonov, 1999, G. Dorokhov, 1996, T. Demicheva, 1994).
The acidotic crisis is not always pronounced, therefore, the following indicators (in addition to above-mentioned clinical signs) can be used to determine the time of its onset: the rate of body weight decrease, urine acidity and concentration of acetone in exhaled air.
1. Decrease in body weight
After an acidotic crisis, the body begins to use its resources very sparingly. In the initial days of fasting, daily weight loss amounts to approximately 1 kg, and after the crisis, the rate of decline slows down sharply (see Fig. 1a). The day of the crisis can be determined by the step on the chart.

Figure 1a and 1b
Changes in urine acidity and the rate of body weight decrease during water fasting (the most distinctive data of one of the patients). In this case, the acidotic crisis occurred on day 7.
(Source: M.V. Ashikhmina, Automated support medical decision system for the management of therapeutic fasting based on the Nakatani method, Abstract of Candidate’s Dissertation, St. Petersburg, 1998.)
2. Urine acidity
Prior to the acidotic crisis, urine acidity increases, and afterwards, it begins to decrease.
Monitoring urine pH with regular test strips is an easy way to determine when an acidotic crisis occurs (see Figure 1b). Both acidity test strips and urine ketone test strips are available commercially.
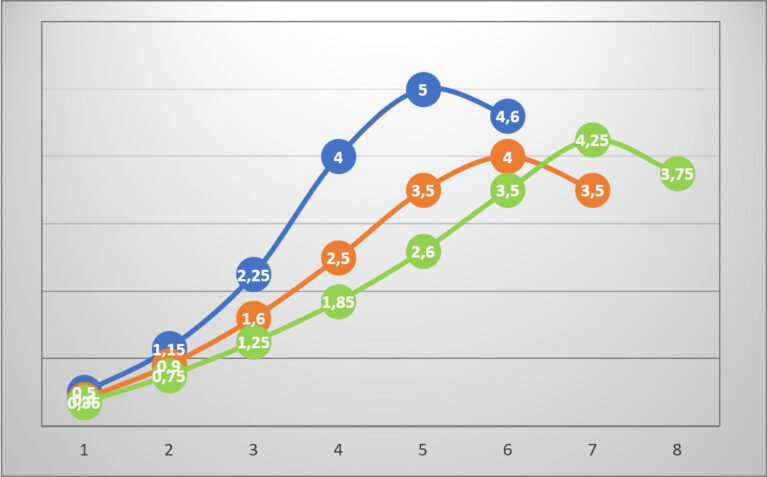
3. The onset of an acidotic crisis may be indicated by the change in acetone content in the exhaled air (see Fig. 2). The maximal points on the curves corresponds to the day of the acidotic crisis onset.

Fig. 2 Dependence of acetone concentration in expired breath condensate on the duration
of water-only fasting:
1 – healthy volunteers with normal weight;
2 – patients with excessive weight;
3, 4 – patients with normal weight
(Source: I.B. Belyaeva. Clinical and laboratory assessment of efficiency of short-term
courses of therapeutic fasting in the early stages of bronchial asthma. Summary of dissertation
for the degree of M.D., St. Petersburg, 1992)

Recently, devices that allow to measure ketone levels in your breath at home became available on the market. They are similar to breathalyzers in appearance and ease of use. However, it does require some skill to get reliable data from them.
To summarize the above: during prolonged water fasting, you need to carefully monitor
your clinical signs and use them to determine the current fasting stage. We must strive to reach
the acidotic crisis and, preferably, complete the third stage of fasting. Then comes the time to
break fasting. Identifying the signs of the completion of the third stage is very important because if they go unrecognized, subsequent fasting will no longer be therapeutic, but damaging, and will lead to the depletion of vital organs by the body (P. Avrorov, V. Pashutin).
An acidotic crisis usually occurs on day 2-4 with dry fasting, and on day 5-8 with water fasting. The third stage ends on day 7-9 with dry fasting, and day 20-30 with water fasting.
These terms are very individual and depend on the patient’s condition, the presence of concomitant pathologies, and even on the previous fasting experience: those who have fasted in the past reach the acidotic crisis faster (Sergey Filonov, 20 Questions and Answers about Dry Fasting).




